
By Toni Wilken (Meditech), Vice Chair, Quality Measures Workgroup
Creation of the proposed Addressing Social Needs (ASN) electronic quality measure (eCQM) supports the important goal of addressing an unmet need in patient care by helping to improve screening and coordination with local and community-based resources. However, the EHR Association has identified several issues with the measure as proposed by its developer, Yale New Haven Health Services Corporation–Center for Outcomes Research and Evaluation (CORE), which we shared recently in our response to CORE’s call for comments.
ASN eCQM
Briefly, the Centers for Medicare & Medicaid Services (CMS) engaged CORE to develop a re-designed measure to evaluate how well hospitals were screening for and following up on the social needs of their patients. The result was the ASN eCQM, which is designed to measure screening of patients for social needs within four domains – food insecurity, housing insecurity, utility insecurity, and transportation insecurity – as well as if an intervention activity is performed.
As noted by CORE in its project overview: “Addressing social needs can improve health and wellness and advance health equity. This measure aims to support hospital initiatives to address the unmet needs of their patients through better screening and coordination with local and community-based resources and enable more public transparency and hospital accountability for whole-person care.”
This measure aims to support hospital initiatives to address the unmet needs of their patients through better screening and coordination with local and community-based resources and enable more public transparency and hospital accountability for whole-person care.
It seeks to build upon existing measurements by:
- Enhancing the accuracy of measurement by refining social need domain definitions and requiring technical standards for endorsed screening tools;
- Promoting efficiency and alignment across the ecosystem through the use of all-payer eCQMs;
- Aligning with national health information technology interoperability standards (USCDI); and
- Encouraging follow-up when screening is positive.
Although it is being developed initially for the Inpatient Hospital Reporting (IQR) program, CMS is expected to include it in other programs like the Merit-based Incentive Payment System (MIPS), Medicare, and Hospital Outpatient Quality Reporting (HOQR).
Scoring Concerns
One of the primary concerns that arose from our review of the proposed measures was with the current point system – which isn’t currently used in any existing eCQM. Specifically, the points don’t necessarily reflect the information that the measure seeks to gather and they lack an opportunity to mine granular data. That will become particularly problematic upon the move to FHIR-based quality measurement, which will increase the diverse analytic uses of the raw data that is captured for measurement.
As proposed, the grouped scoring allows for significantly uneven representation with limited insights. A hospital could have fewer patients with high scores and many patients with low scores and they would balance out. Or, if one hospital has a high incidence of food Insecurity and another has a high score for housing Insecurity, but they both have an average score of 20, it is impossible to know how they are performing in each domain.
Thus, to achieve greater nuance, we recommend adopting a methodology that more closely resembles a standard eCQM measurement in which granular data helps glean a greater understanding of the nuance of a given population. eCQMs have proven to be highly effective at mining data and putting forth meaningful scores when the measures are written with the appropriate numerators, denominators, exclusions, and exceptions.
Further, we recommended that CORE consider using a standard denominator/numerator style measure, a scoring method that provides more precise screening and is familiar to developers and hospitals. The measures should include stratifications for each domain that are similar to the SDOH-1 (screened), SDOH-2 (screened positive), and a potential SDOH-3 (screened positive and followed up). For example:
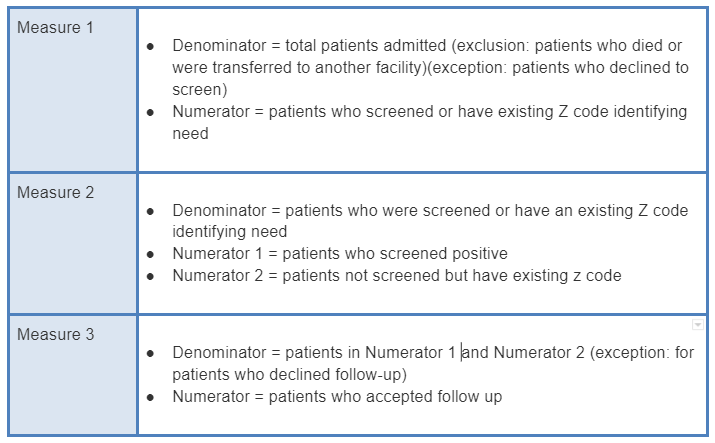
These three measures broken down into denominators, numerators, exclusions, and exceptions would provide more meaningful data and evaluation of patient status and outcomes.
Other Concerns
The EHR Association lays out its concerns and recommendations in several other areas, including the need to include the Interpersonal Safety domain to achieve consistency with existing IQR Program SDOH measures.
We also recommend providing an exception for those communities that lack services to meet the qualifying follow-up needs of any given social domain, which would prevent hospitals and providers in those areas from being penalized. Other recommended exceptions include when patients refuse to answer screening questions and for patients who completed screening but are discharged against medical advice.
Our complete response to the ASN eCQM can be read here.
